For hospital executives and innovation leads, the window to "experiment" with AI is closing. The market has shifted from novelty to necessity. The priority for 2026 is deploying tools that immediately reduce cognitive load and mitigate financial risk.
To navigate the crowded vendor landscape, the focus should be on three specific operational constraints.
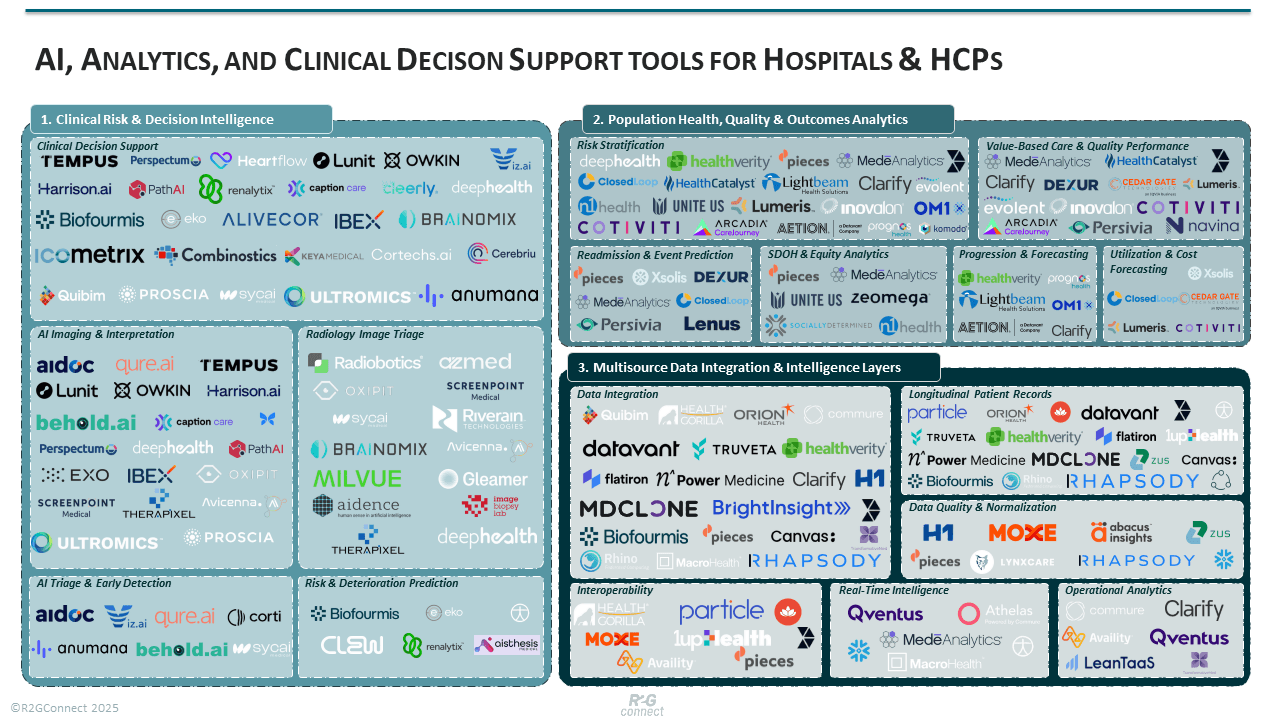
1. The Bottleneck: Cognitive Load & Diagnostic Variability
Clinician fatigue is a safety risk. A radiologist at hour ten of a shift has a different sensitivity threshold than at hour one. This variability leads to delayed detection of deterioration (e.g., sepsis), missed incidental findings, and massive backlogs in imaging. When specialists are buried in routine checks, turnaround times extend, and patient outcomes suffer.
The Solution: Clinical Diagnosis & Treatment Planning Hospitals are deploying AI models to act as a safety net, not a replacement. These tools function as a "second read," automating the triage of normal cases so specialists can focus on acuity.
Representative Use Cases:
- Clinical Decision Support: Systems that provide real-time, evidence-based alerts within the clinical workflow to reduce errors.
- AI Imaging & Interpretation: Computer vision tools that automatically flag abnormalities in X-rays, CTs, and MRIs.
- Radiology Image Triage: Algorithms that prioritize worklists, ensuring critical cases (e.g., hemorrhages) are reviewed first.
- AI Triage & Early Detection: Front-line tools that analyze intake data to predict patient acuity faster than standard protocols.
- Risk & Deterioration Prediction: Background monitoring of vitals to alert rapid response teams hours before a patient crashes.
The Trade-off: These tools reduce variability but introduce "alert fatigue" if not calibrated correctly. Implementation requires rigorous threshold setting to avoid overwhelming clinicians with false positives.
2. The Bottleneck: The "Black Box" of Discharge Risk
Once a patient leaves the hospital, visibility drops to zero. Yet, hospitals are financially liable for what happens next. Without accurate forecasting, care teams cannot distinguish between a patient who will recover at home and one who will bounce back to the ER within 30 days. This lack of visibility drives preventable readmissions and penalties.
The Solution: Population & Patient Forecasting New platforms analyze historical data and social determinants to assign risk scores to cohorts. This moves care from reactive to proactive.
Representative Use Cases:
- Risk Stratification: Segmentation of patient populations to identify high-risk cohorts requiring intensive management.
- Value-Based Care & Quality Performance: Tracking and predicting performance against payer contracts to maximize reimbursement.
- Readmission & Event Prediction: Modeling that identifies patients most likely to return to the hospital within 30 days.
- SDOH & Equity Analytics: Integrating non-clinical data (housing, food security) to address barriers to care.
- Chronic Disease Progression & Outcome Forecasting: Predicting the trajectory of long-term conditions to intervene before acute episodes.
- Utilisation & Cost Forecasting: projecting future resource needs and cost drivers across the patient population.
The Reality Check: Data is only as good as the intervention it triggers. Identifying high-risk patients fails if the hospital lacks the care coordination staff to act on the insight.
3. The Bottleneck: Data Fragmentation
You cannot analyze what you cannot see. A patient’s MRI is in the PACS, vitals are on a bedside monitor, and history is in the EHR. These silos prevent real-time intelligence. Clinicians spend valuable time hunting for information across disjointed systems, and advanced AI models fail because they lack access to a unified data stream.
The Solution: Data Integration & Analytics Infrastructure solutions are emerging to unify disparate sources into a single, usable analytics layer. This is the "plumbing" required before any advanced AI can function at scale.
Representative Use Cases:
- Data Integration: Middleware that connects siloed systems (EHR, Lab, PACS) into a coherent ecosystem.
- Longitudinal Patient Records: Creating a single, continuous view of a patient’s history across all sites of care.
- Data Quality & Normalisation: Cleaning and standardizing messy data to ensure it is usable for analytics and AI.
- Real-Time Intelligence: Dashboards that display live clinical or operational data for immediate decision-making.
- Interoperability: Solutions ensuring seamless data exchange between different vendor systems and external partners.
- Operational Analytics: Tools that optimize hospital flow, bed management, and resource allocation.
The Constraint: This is the heaviest lift technically. It requires significant upfront investment and often faces resistance from legacy vendors protecting their proprietary ecosystems.
A Call for Innovators
Do you have a solution that solves these specific hospital bottlenecks? Leading hospitals are actively seeking partners in Clinical Diagnosis, Population Forecasting, and Data Integration right now. R2GConnect has launched a global open call for Analytics, AI & Decision Support Systems. This is your opportunity to bypass cold outreach and pitch directly to hospital innovation teams seeking commercial partnerships, pilot projects, and funding.
Don’t miss your window to bring your technology to the frontline of care. Apply Now: Analytics, AI & Decision Support Systems Open Call.